
Neonatal Jaundice - The physiological jaundice in newborns
There are many moments in our career in healthcare, that make us really satisfied.
A successful surgery, seeing the defib monitor showing signs of cardiac activity after a successful CPR, and the cry of a baby immediately after birth. If you have already, then you know what I'm talking about. But if you haven't, trust me. It does live up to it's hype.
But there are times when we are brought crashing back to reality. One of those times is when an anxious mother brings a seemingly healthy newborn to you with a complaint. This time with yellowish discoloration of the skin of the face and the eyes.
We know it's jaundice. Getting there is the easy part. What we are not sure is what we need to do after that. The parents are waiting for an answer.
The answer to that question is precisely what we are going to address in this article - Neonatal jaundice.
A fairly common entity. But the importance lies in the subtle but distinct differences between the physiological and the pathological variants.
When faced with a doubt, stick to the basics:
History. Examination. Then investigations. Always.
So let's go back to the anxious parents who are sitting in front you. Some basic questions reveal that the the child was doing fine after birth, feeding well, active. On the 6th day, the mother noticed yellowish discoloration of the eyes. Next day it's on the skin of the face and neck. Since it hasn't disappeared, she's brought the baby to you.
Now you examine and sure enough, there's yellowing of the skin upto the neck. Otherwise your examination is unremarkable. You want to confirm this so you ask for the bilirubin levels with both conjugated and unconjugated fractions. The report comes, you're happy with it. You reassure the parents, and send them off with some advice.
From this, we need to understand that physiological jaundice has some typical characteristics.
- It never appears within the first 24 hours after birth.
- Rarely lasts over 2 weeks.
- Total bilirubin is less than 15 mg/dL.
- The direct(conjugated) bilirubin fraction is within normal limits.
Before we begin to understand the basis of this happening, it makes sense to remind ourselves the origin story of bilirubin.
Bilirubin is a product of hemoglobin metabolism. More specifically, the heme part of hemoglobin. When RBCs get destroyed, the hemoglobin that gets released into circulation separates into its components: heme and globin. Globin gets dismantled and joins the protein pool; heme gets progressively metabolised to eventually form bilirubin.
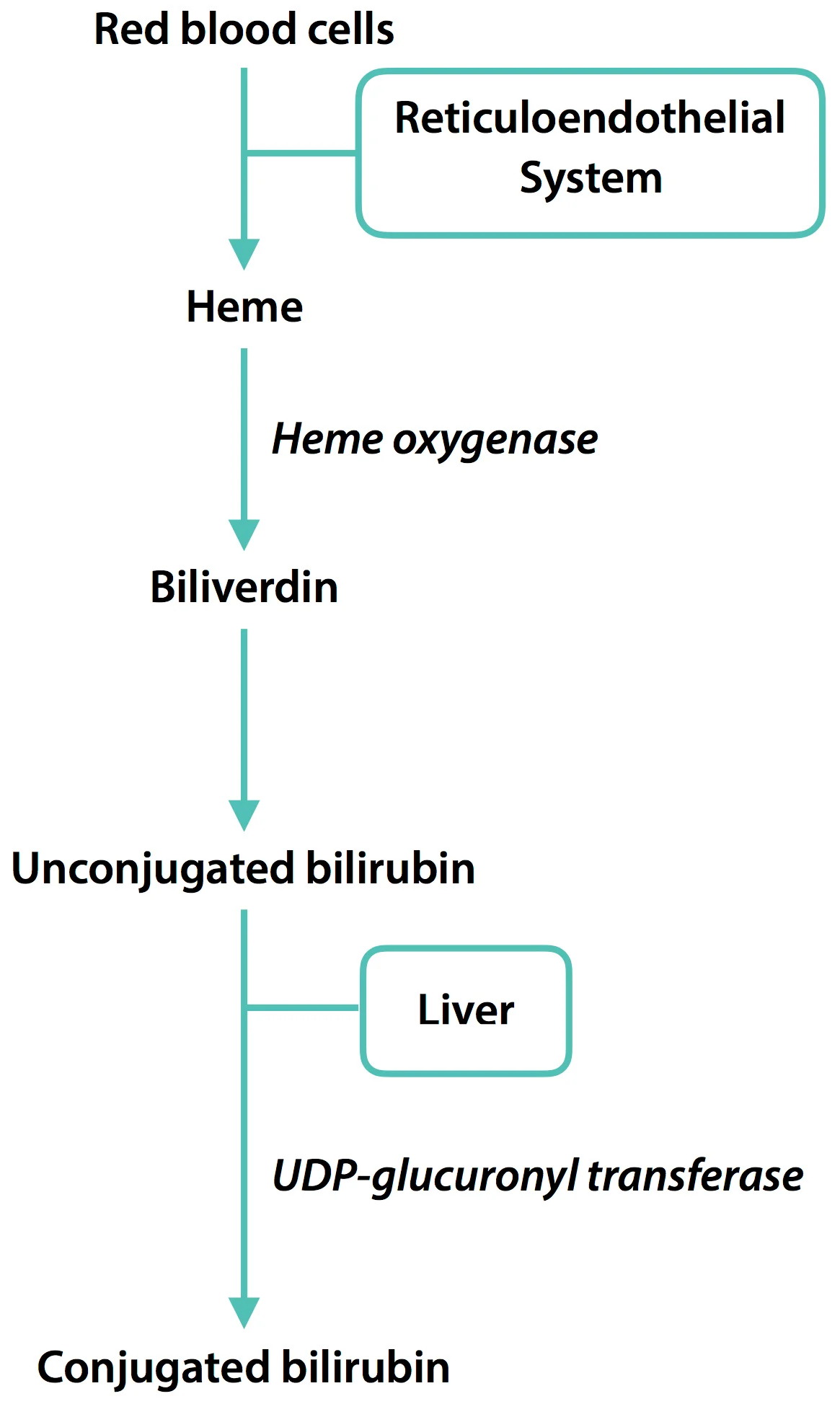
Now the bilirubin formed isn't soluble, so as soon as it's formed, it flocks to albumin (a plasma protein), and this is carried to the liver. The big boss of the body.
In order for this bilirubin to be excreted it needs to be made soluble. That's where the liver adds a glucuronyl group to the bilirubin by an enzyme called “Glucuronyl Transferase”, a process called conjugation.
This conjugated bilirubin can now be excreted in the bile where it undergoes some more changes and eventually gets excreted either via the stools or urine.
Normally the levels of bilirubin in the body are between 0.2-1.2mg/dL of which the conjugated fraction ranges from 0-0.3mg/dL, the remaining being the unconjugated bilirubin.
Now we might wonder..
Jaundice is a pathological process. Why is it called “physiological jaundice” then?
Basically, in the newborn baby's body, there are certain normal processes that can lead to this condition.
Newborns have around 5.1- 5.3 million RBCs per cubic millimetre, and the usual lifespan of these cells are between 60 to 90 days. Comparing that with a normal adult who has about 4-5 million RBCs per cubic millimetre, with an average lifespan of 120 days, it's easy to understand that these cells lyse pretty easily and a lot of them lyse and hence, and a lot of bilirubin is formed. That is, they have an increased cell turn over rate.
Ideally all of them should be conjugated and excreted. But in many neonates, these processes at the liver are still immature. Each gram of Hemoglobin that gets broken down forms 35mg of bilirubin; so it's logical to understand that the liver gets overwhelmed by the sheer amount of bilirubin it needs to process, and hence, jaundice is produced.
Since the bilirubin produced cannot be conjugated, it's also logical that the unconjugated fraction is elevated; the conjugated bilirubin levels are normal in physiological jaundice of newborn.
We might ask ourselves.
Why do we need to know so much about this seemingly benign condition?
This unconjugated bilirubin, if you recall, is bound to albumin while being transported to the liver for it's metabolism. To be more specific 25mg of free bilirubin gets bound to albumin tightly, in every 100ml of plasma. This is an effective buffer system; so when the plasma concentration is very high, even this buffer system fails. Free unconjugated bilirubin can cross the blood brain barrier of the baby and cause neuronal damage which is called “kernicterus”; the prognosis for such babies isn't very good, so we need to identify jaundice earlier and start treatment if necessary.
So there you have it. Physiological jaundice.
We’ll be looking at what pathological jaundice is, how to approach and how to manage these babies in the next article.
Author: Anirudh Murali (Facebook)
Sources and citations
1. Agarwal, Ramesh K, et al. “Chapter- 8: Newborn Infants.” OP Ghai's Essential Pediatrics, 8th ed., CBS Publications, pp. 172–176.
2. John E. Hall, "Chapter 70 - The Liver as an organ", Guyton and Hall Textbook of Medical Physiology, 12th Ed, Elsevier-Saunders publications, pp. 840-842
3. Victor W. Rodwell & Robert K. Murray, "Chapter 31 - porphyrins and bile pigments", Harper's Illustrated Biochemistry, 30th ed., Mcgraw Hill- Lange Publications, pp. 330-332