
Porphyria - The Royal madness that freed America
King George III is still remembered and mocked for chasing thirteen American colonies out of Britain’s puissant empire, making The United States of America an independent nation. What was it that caused this otherwise successful British emperor, who had won the Seven years’ war against the French and made his empire the world’s greatest colonial power, go nuts during the later part of his life?
His recurrent transient illness would typically begin with an abdominal discomfort, that then progresses to a severe colicky pain, cramps and rashes. The 18th century royal physicians would prescribe their usual remedy for abdominal pain, an emetic ‘tartar’. Subsequently, his pain would become debilitating, eyes yellow, legs swollen, urine brown and mental illness would ensue. During these periods of insanity, his majesty appeared to be hallucinating, assaulting his family, physicians and chasing ladies in his courtroom.

King George III
Only years after his death, scientists suggested that His Majesty had been suffering from porphyria, a rare genetic metabolic disorder in heme biosynthesis.
About 85% of heme is synthesised in erythroid precursor cells in the bone marrow necessary for hemoglobin and the majority of the remainder in hepatocytes for cytochrome enzymes. Accordingly, porphyrias are classified into two groups — hepatic and erythrocytic, depending on the site of overproduction and accumulation of the porphyrin precursors — liver and bone marrow, respectively.
Hepatic porphyrias usually manifest in adulthood as transient attacks of neuropathic abdominal pain, peripheral motor neuropathy and mental disturbances with these attacks often precipitated by dieting, certain drugs or hormones. In contrast, erythropoietic porphyrias generally manifest in early childhood as cutaneous photosensitivity.
A little knowledge on the process of heme synthesis will help us understand the disease better.
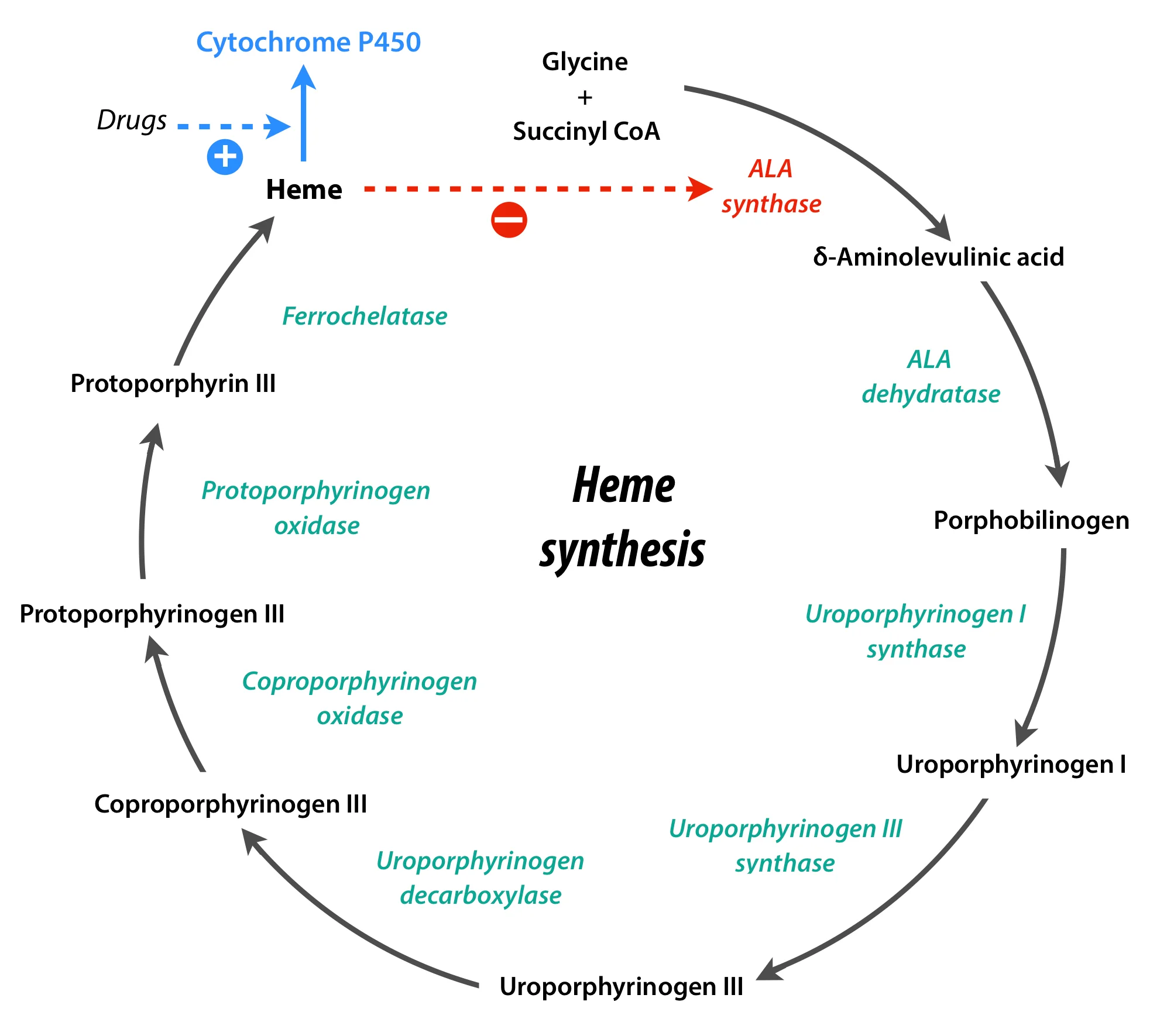
Regulation of heme synthesis in the liver happens at the level of ALA synthase 1 (ALAS1). The rate of synthesis of this enzyme increases in the absence of heme, but diminishes in its presence, thus keeping the hepatic levels of heme under check. Heme in the liver is utilised for production of cytochrome P450 enzymes. Now, the glitch is, certain drugs that stimulate cytochrome enzymes also have to stimulate ALA synthase production and thereby heme production for the very bright reason that these cytochromes need heme for their manufacture.
Imagine what would happen when ALAS1 is stimulated but another enzyme down in this process is deficient. The precursors formed before the deficient enzyme would accumulate, right? This is the patho-biochemistry behind the disease. Different types of porphyrias are named based on the enzyme deficient.
One good example is Acute intermittent porphyria, in which uroporphyrinogen I synthase is deficient that accumulates δ-aminolevulinic acid (ALA) and porphobilinogen (PBG) in the body fluids and tissues. Because of the structural similarity of δ-aminolevulinic acid to γ-aminobutyric acid (GABA), its accumulation may impair GABA function, leading to the neuropsychiatric symptoms. Another mechanism described is the direct toxicity of the precursors to CNS tissue. These precursors can also cause axonal degeneration in the PNS leading to peripheral motor neuropathy.
This is not the only mishap that occurs when an enzyme below in the synthetic process is impaired. Let us consider Porphyria cutanea tarda in which uroporphyrinogen decarboxylase is lacking. Here, another class of compounds called porphyrinogens (Uroporphyrinogen I & III) accumulate in addition to ALA and PBG.
The problem with porphyrinogens is that they spontaneously oxidise to give porphyrins that are both photosensitive and coloured. Due to their photosensitivity, they react with oxygen in light, generating oxygen radicals that injure lysosomes and release degradative enzymes which cause skin damage and scarring. The colour of porphyrins is the reason behind urine turning purplish-red on standing.
Going back to King George III, the flaw in his tale lies with the compound ‘tartar’ prescribed by his physicians. The beauty of tartar is that it contains arsenic which is a cytochrome P450 inducer.
Without doubt, the poor patient of porphyria was iatrogenically made insane.
Though, the victory of the US over the British, was whether due to the valour of the US army or due to the British king’s madness is debatable, the role of the royal physicians can never be forgotten in bringing down the once invincible British empire!
Author: Anten (Facebook)
Sources and citations
Victor W. Rodwell and Robert K. Murray. “Porphyrins & Bile Pigments” Harper's Illustrated Biochemistry. 30th ed. New York: McGraw-Hill Education, 2015. 323-30. Print.
Robert J. Desnick and Manisha Balwani. “The Porphyrias” Harrison’s Principles of Internal Medicine. 19th ed. New York: McGraw-Hill Education, 2015. vol. 2, 2521-2530. Print.
Jennifer A. Tracy and P. James B. Dyck. “Porphyria and its neurologic manifestations” Handbook of Clinical Neurology. 120th ed. Elsevier, 2014. 839-845. Print.