
Gut Rotation - The Twist of Fate
The gut is one of the most intricately engineered structures in our body. Like every other organ, the gastrointestinal tract has also gone through an evolutionary roller-coaster over millions of years. The current day stomach and intestines have evolved to be a highly energy efficient system and break down every last bit of what we eat and sustain life. So how do these structures come into being?
The entire gastrointestinal tract (GIT) develops from a single long tube extending from the cranial to the caudal end of the embryo.
This gut tube is an endodermal tube and gives rise to the future mucosa of the GIT. The mesoderm surrounding the tube differentiates into the other histological layers of the GIT – namely the lamina propria, submucosa and the muscular wall giving additional strength and structure.
The gut tube is closed on either ends:
Cranially it is closed by the buccopharyngeal membrane which seperates the primitive mouth from the pharynx.
Caudally the tube is closed by the cloacal membrane which later disappears to form the openings of anus, urethra and vagina.

The tube is divided into 3 distinct regions based on the arteries supplying them:
- The foregut is supplied by the celiac artery
- The midgut by the superior mesenteric artery and
- The hindgut by the inferior mesenteric artery.
These 3 arteries are unpaired branches from the abdominal aorta.
The foregut develops into the pharynx, esophagus, stomach and the proximal duodenum. The gut tube progresses to grow in length, especially the mid gut segment, after the 4th week of intrauterine life. The midgut develops into the future distal duodenum, small intestine, ascending colon and transverse colon. What’s interesting to note is that, the length of the small intestine is more than twice the length of an infant.
If thats the case, how is such a long tube accommodated within a small fetal abdomen?
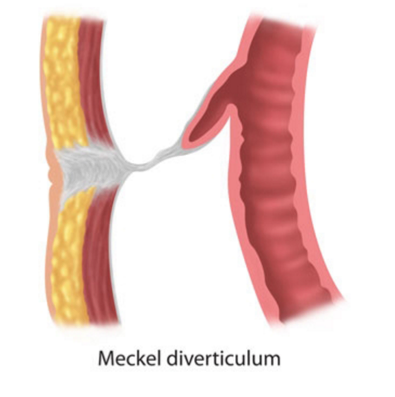
It is possible by a process called physiological herniation. Around 5th week of the intrauterine life, the growing midgut lengthens more rapidly compared to the growth of the abdomen. The limit in space is only made worse by the rapidly growing liver and speen. Hence the growing midgut is thrown into a U shaped loop and pushed out of the abdominal cavity into the umbilicus. The upper limb of the U is destined to be form the future small intestine and the lower limb forms the ascending and transverse colon. At the tip of the U, the midgut is attached to the umbilicus by a thin duct called the vitellointestinal duct which disappears during the later stages of development. The space between the 2 limbs of the U has the mesentry – a fan shaped structure that holds all the loops of intestine together. The superior mesenteric artery which supplies the midgut structures passes through the center of the U within the mesentry. If the vitellointestinal duct fails to disappear, it might get obstructed and cause intense abdominal pain in children – a condition diagnosed as Meckel’s diverticulum which needs surgical excision of the duct.
It is interesting to note that the surgeon will always locate the Meckel’s diverticulum along the antimesentric border of the small intestine (opposite to the edge of attachment of the mesentry) simply because of its anatomical position during development.

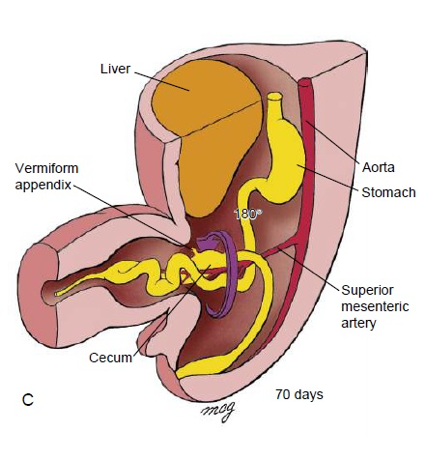
Between 6th to 10th week as the U loop further herniates into the umbilicus, it undergoes 3 rotations in a step wise manner. First it rotates by 90° in the anticlockwise direction (as seen from the front) along the axis of the superior mesentric artery. At the end of this first rotation the upper limb of the U, or the future ileum comes to lie on the fetus’s right and the lower limb of U or the future colon lies on the left. If development arrests at this stage such an adult would have all the loops of small intestine on his right and the colon entirely on his left – an anomaly called non-rotation of the midgut.


Non-rotation : Barium study showing small bowel loops predominantly on the right and ascending colon on the left
At the end of 10th week, the midgut retracts back into the abdominal cavity. Though the reason for this retraction is not exactly known, the midgut undergoes an additional 180 degrees anticlockwise rotation. The net rotation of the entire midgut is 270° anticlockwise (90° + 90° +90° ). This brings the ceacum (developed from the lower limb of the U) to the right side. If the midgut rotates 180° clockwise instead of anticlockwise, then the net rotation would be 90° clockwise (90° - 180° = -90°). This anomaly is called reverse rotation of the gut. The small and large intestines are spatially oriented to each other normally with one exception – the duodenum lies in front of the transverse colon rather than behind it.
Normal Rotation

Reverse Rotation
Under rare circumstances, the upper limb of the U might only undergo the 1st rotation and the lower limb of U might only undergo the 2nd and 3rd rotation. The result of this uncoordinated malrotation can be catastrophic. The ceacum gets fixed in the midline below the stomach. The duodenum or the ceacum may get suspended from the dorsal body wall by a thin abnormal band of mesentry called Ladd’s band. Such a ceacum or duodenum is prone to get twisted around this narrow band of mesentry leading to acute obstruction. Patients with such malrotated guts present to the emergency with acute abdominal pain and often the obstructed segment of gut would be necrosed and may not be salvaged.

Mixed Rotation
These anomalies of gut rotation are quite rare entities in clinical practice. The fact that a newborn is born with absolutely normal structures at most instances can only be best explained as nature’s magic at work. However, as doctors, the possibilities of such oddities must always be borne in mind!
Author: Soundarya V (Facebook)
Sources and citations
Gary C. Schoenwolf, et al. “Chapter 14 - Development of Gastrointestinal Tract.” Larsen's Human Embryology, 5th ed., pp. 341–361.