
Parkinson's - A debilitating depletion of dopamine
He was The Greatest.
A record 22 heavyweight titles in the history of modern boxing, a prominent voice in the American civil rights movement, a freestyle rapper, an actor on Broadway musical...an eccentric personality whom the world watched gradually being reduced to a man with a mask like, expression less face with uncontrollable tremors of his hands. This was the story of Muhammed Ali, truly The Greatest, both inside and outside the boxing ring. But some believe his greatest battle was not inside the boxing ring, but rather in real life, fighting Parkinson’s disease for over decades.
With growing awareness about the disease, some of you might know that Parkinson’s disease is due to depletion of dopamine in the brain. But how does a low level of dopamine lead to such dramatic clinical features?
Imagine going out for a jog on a misty Sunday morning. Or trying to strum your favourite song on that ukulele. These simple pleasures often have the most complicated mechanisms of execution in the body. Any voluntary movement in the body is planned in the Premotor cortex and is performed by the Pyramidal pathway - a series of neurons originating from the pyramidal cells (also known as Betz cells) of the motor cortex, traversing the internal capsule, decussating to the opposite side in the medulla and terminating on specific spinal segments. These motor actions are further perfected by another circuit of neurons called the Extra-pyramidal tracts. One of the major components of the Extra-pyramidal system is the Basal ganglia, which is a cluster of nuclei arranged on either side of the lateral ventricles. So your desire to jog is accomplished primarily by the motor cortex and pyramidal pathway. But the Extra-pyramidal system controls the intensity of movement in the muscles involved in jogging and facilitates the movement.
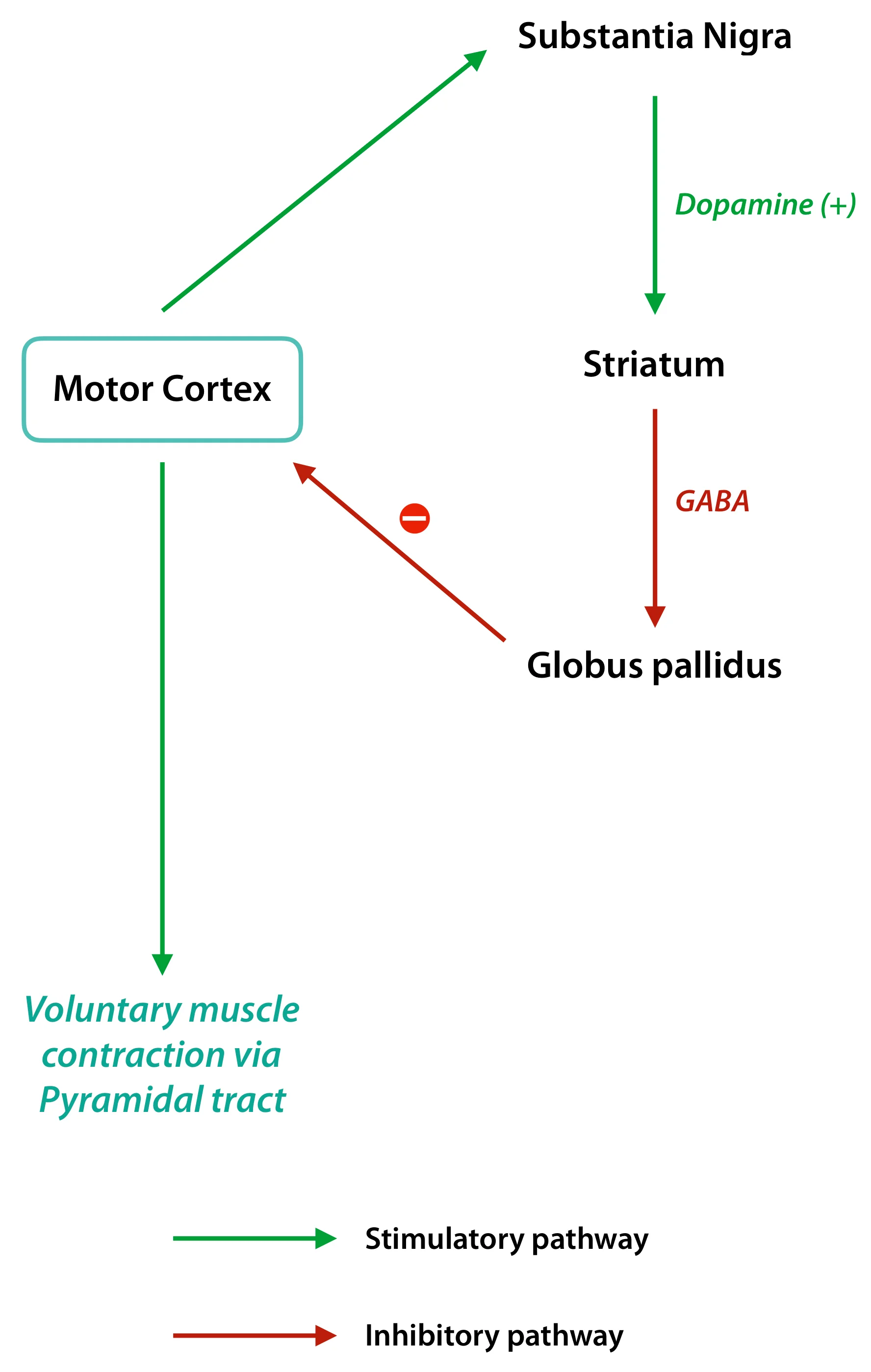
The Basal ganglia is made of the Caudate, Putamen, Globus pallidus, Substantia nigra and Subthalamic nucleus. All these nuclei are connected to each other as well as to the motor cortex via multiple intricate neuronal circuits. However what is important to remember is the Caudate and Putamen, together known as the Striatum serves as the main input for all signals reaching the Basal ganglia while the Globus pallidus is the major output center. The Substantia nigra is the major source of dopamine in the brain. Dopamine being an excitatory neurotransmitter, activates the striatum (input center). The Striatum controls the Globus pallidus through inhibitory neurotransmitter like GABA. Hence activation of the striatum actually inhibits the Globus pallidus. And here’s where things get interesting. The output from Globus pallidus to the pyramidal pathways is also via inhibitory neurotransmitter GABA. A state of double negatives exists here – the striatum inhibits the Globus pallidus whose main function is to inhibit the motor cortex. Like elsewhere, double negatives make a positive. The inhibitory control of the Globus pallidus over the motor cortex is abolished by the activation of the striatum and hence the basal ganglia, as a whole, ultimately facilitate voluntary muscle contractions. In a state of dopamine deficiency, the striatum loses its control over the Globus pallidus. Excessive GABA firing from the Globus pallidus leads to reduced activation of the motor cortex and parkinsonian features like muscular rigidity, involuntary tremors and postural instability. In severe forms of the disease, the patient is often in a state of akinesia having serious difficulty in initiating voluntary movements.
All treatment modalities available for Parkinson’s are aimed at increasing the level of dopamine. Arvid Carlsson, a Swedish neuropharmacologist first demonstrated the benefits of administering L-DOPA in the 1950s. It was a groundbreaking discovery that rightfully earned him a Nobel prize almost 50 years after the discovery. However direct oral or IV administration of dopamine does not have any clinical significance because it does not cross the blood brain barrier. L-DOPA has subtle structural modifications which enables it to cross the blood brain barrier. Surgical modalities like deep brain stimulation have shown to improve akinetic symptoms. Deep brain stimulation involves placement of electrodes in specific parts of the brain parenchyma which stimulates specific centers, similar to cardiac pacemakers. Newer experimental therapies like transplantation of fetal substantia nigral cells and gene therapies hold a promising future for people fighting this debilitating disease.
And that’s how complex neuronal circuits make simple activities in life possible.
Author: Soundarya V (Facebook)
Sources and citations
C. Warren Olanow, et al. “Chapter 449 - Parkinson's Disease and Other Movement Disorders.” Harrison's Principles of Internal Medicine, 19th ed., vol. 2, pp. 2609–2618.
John E. Hall. “Chapter 56 - Basal Ganglia - Their Motor Functions.” Guyton Textbook of Medical Physiology, 12th ed., vol. 1, Saunders-Elsevier, pp. 689–693.